So San Milan says LT1 is the threshold he targets for “Zone 2” upper limit.
Maffetone specicially says “one cannot obtain the max aerobic heart rate by measuring blood lactate or AT”
Which to me says Maffetone thinks lactate is poor for determining the level you train at to stay in optimum fat burning. But he does clarify “respiratory quotient (RQ) is an effective treadmill test that provides athletes with the percent fat and sugar burning at various heart rate.” Which obviously makes sense. Measuring fat your buring percent is a good indicator of the ratio of fat you are buring So I see this as Maffetone saying their is a clear relationship between HR and RQ. I have not seen San Milan talking about RQ, and to my limited brain since we are talking about fat burning that is the most obvious indicator.
San Milan discusses on multiple forums that LT1 is where it is not so easy to talk and Maffetone is clearly indicates his hr aeroobic threshold is at a lower level.
@Ratz Do you have any experience with different methods of testing. Do you use other indicators outside Maffetone’s formula’s especially because Maffetone states 65+ his formula does not work.
I’m not in full agreement here…
The article is from 2015 and the situation regarding cost and knowledge is no longer the same.
Lactate meters are now relatively inexpensive. For a coach using them on multiple athletes, the cost is really low. For advanced amateurs interested in all the physiological stuff, the cost is comparable to a main stream head unit.
RQ measurement on the other hand is very expensive and can only be done in a lab on a met-cart. And you should specifically tell the tester that you want a test that identifies AeT and not just do a CPET test. A max effort test is almost always done to target VO2max and there is not enough time at the beginning, warm-up, to come to that first steady state that is so important to allow deducing AeT. You start exercising by using predominantly carbs, RQ about 1 and the ramp test kicks in after 10-15 minutes. That’s too soon, because you first need to make your body switch to a fat burning state and that takes on average 15-20min. They should wait until your RQ drops to around 0.7, value at which fat is the main fueling substrate. Only then should the ramp be started. And during VO2max testing, the ramp is way too fast to allow proper identification of AeT. Any decent amateur will have a ramp with 20-25 W per minute. Totally inadequate to test for AeT…
The testing protocols for lactate on the other hand are now mainly optimized for AeT testing. You start at very low intensity and stay there for at least 20 minutes, preferably even 30 minutes. Take a first lactate measurement at 5 min and then about every 6 min. Lactate should go down because you switch from carb/glycolisis system to more and more fat. The more fat the lower the lactate because fat burning is not producing lactate and any lactate still in the blood will be used as fuel during that low intensity phase. Then you start a slow ramp or step protocol and keep measuring lactate every 6 min. The lactate curve will do something very similar compared to the RQ curve. Lactate will first lower to ‘base level’ during the first steady state low intensity. RQ will evolve from around 1 to around 0.7. When the ramp or step is started, both will go up. Now forget about any pinpoint numbers like 2 mmol and the like. What you’re looking for in lactate is the first significant slope change or the point where the lactate is 1 mmol above base level. The rising lactate indicates more carb usage, just like the rising RQ that will return to 1, indicating a more carb dominant fueling.
If you want to get anaerobic threshold by lactate and/or RQ, I would advice to not do that in the same test. For AT/VO2max, a steeper ramp test is needed.
During the lactate test, stop when lactate has gone 3-4 mmol above base level. That’s plenty to have a lactate curve that you can follow up during base period. If you do your training in the right way, the curve should move to the right when plotted against Power, and on longer term even when plotted against HR.
I understand your thinking that lactate testing is easier now, what I believe Maffetone was saying is it is not accurate for aerobic threshold and he feels aerobic threshold aligns with RQ. As you know just because it is easy does not mean it’s accurate representation of a secondary body state. And I don’t know if we have advanced that much since 2015 in lab testing of LT1, VT1, and RQ. I realize home tests have advanced infinitely.
I also realize you are thinking (and others are saying) lactate aligns with VT1 which means either that Maffetone was just wrong, or his lactate tests were inaccurate. I just have not been able to find clear evidence of what you are saying is true but maybe it exists (you got anything?) I see evidence indicating it for lt2/vt2 accuracy. I have no idea if Maffetone is right or not it just the data dispelling his suggestion looks pretty fuzzy to me at this point.
I have also seen many graphs like this below. Which it would be pretty hard to say 2.0 is the actual turn point. Really in this example it more clearly starts going up either at 1.9 or 2.2 not 2.0.
Just search google images and you see all kinds of different graphs and each look enough different that while 2.0 might be an average and semi reasonable predictor, it might be likely saying 220-age is a reasonable predictor.
I don’t know if what I am saying is true. I just threw this idea out there as a discussion point. I know you have researched this more than me. I am just presenting what I see. I am trying to meet with Andrea on this too. I pretty sure at Mapei they test all 3 markers on the pros and have been for 20+ years so he might have some additional insight. I am not sure if they actually cared that much about LT1 / VT1 though but he might have some additional graphs or thoughts on this.
Not to throw any other wrench in this but Coggan says in recent interview it is all BS and their is no LT1 turn point it’s just a continuum. He talks very good but I think he can come to the wrong conclusion at times… (can’t we all) After what I call his TSS/sweet spot failure, in general don’t use his advice for the most part but I am sure he is right in many things. He seemed to be dispelling this Zone 2 training at some level or that was my interpretation of what he was saying. But I say TSS failure, I think it was a success really but it just turned the wrong way.
Now I have no idea if SMO2 means anything, but the guys at Moxy thinks it really can be accurate for VT1 (in some individuals). And I can say the first turn point is incredibly obvious in my testing. Here is an example. You can see oxygen levels dropping like a rock at ~130bpm.
To be clear, I am 100% in agreement that the most exact way of identifying the fat-burn zone is with RQ. But I mentioned quite some disadvantages like cost and knowledge of protocol to use. Let’s face it, if you go to a lab for sports oriented testing, the N° 1 priority for the testing facility is sadly still to make money with it…
I am in hospitals daily as a service technician for diagnostic equipment and the most important thing is that the device ‘functions’, as in ‘spitting out a document’ that proofs that the exam was done. Because that is the decisive point that makes the money come in. I’ve seen so many cases where the results on the document are simply the result of recording environmental noise. In most cases, the patient doesn’t need that exam, but it was done simply to make money. Not really harmful for the patient, but a practice that is making health-insurance more and more costly.
What I was saying about the lactate curve is mostly sourced from Alan Couzens and Gordo Byrn. They are mainly following Maffetone, but are using more modern technology. The core message is very much like Maffetone. The user-friendliness of modern lactate meters has significantly improved and the results are much less error-prone.
I am about to buy my lactate meter and will surely post my experiences with it.
On the point if AeT is the same as the lactate inflection point: I don’t know. But AeT is not the same as FatMax either… What we do know, is that they are all quite close, as in a couple of beats. And your MAF zone is 0-10 beats below the MAF HR. So why are we chasing that exact HR number? Just make sure that you stay approximately 3-5 beats below for the majority of the time and you will be good. But the problem is once again that this is so painfully slow when you start doing it, that everyone trying it out wants to go as high as possible. So they mis-use the formula or use some other test method that gives a higher result. Totally defeating the purpose of the MAF system.
I have absolutely no knowledge about SMO2 measurements, so I’m not going to comment on that.
The actual situation is that there are a number of different methods that return very similar results. That on its own, should make us more confident that this AeT point is really a physiological marker.
Yes we are in complete agreement as always. I follow Couzens on twitter (one of very few people) but I have not read into his opinion on this stuff. I don’t know Gordo. So we don’t have RQ and if we got tested their is reasonable chance it is whacked (your expertise) unless we can go to Mapei, assuming they have this test. I know, I was just looking at lumen. It’s probably crap. https://www.lumen.me/ I was even thinking about could you use one of these ketosis devices as a fake RQ device… I can’t wait to hear what you find out and see your curves. I need to break out my SMO2 device. They (Humon) went out of business so I kind of lost interest but it should still work.
I am a believer in Maffetone like you, but I think the people that come in listening to San Milan would tend to set it about 10 beats higher, which might work as well but according to Maffetone it won’t in a fair number of people. So they will try San Milan’s Z2 and say it does not work. Also Maffetone does not work for 65+ and I have a fair number of 60-65+ guys contact me via email. Even 60 could start getting more iffy. Trying to convince people they should go down by 5 or 10 BPM is like a sin, so I am just looking for ideas for alternatives and would love to see a study of 70% of max HR vs 80% of max HR for 4 months in a bunch of “average cyclists.” Or Maftone vs maffetone +10. Maybe we should create one
Yes for me my breadth test estimate, Maffetone and SMO2 are all in very close alignment (or were about 2 years ago). But Moxy guys said SMO2 his hit or miss, but it’s pretty clear that it works or it doesn’t in specific individuals and I think they thought about 60-70% of the people it worked for. For me 4 out 5 ramp tests were very consistent for the first turn point. More consistent for the first turn point than the second one. I need to test it some more.
Every now and then, we see people reacting that they tried it ‘to the letter’. And they all have the same response: it works!
We need more of those testimonies, but sadly people tend to react more if things don’t work…
Having myself quite a number of years of experience, all I can say is that I perform better and feel better at the same time. The years of going out and trying to crush my PB day after day are long gone. And I’m enjoying my workout time so much more .
Actually there are thousands of people on Maffetone’s FB group saying it works but most are runners and cyclists don’t trust runners I saw a few cyclists on Reddit saying they tried it and it worked. I tried it and it worked as a runner so I fall into that untrustworthy category Also I am so slow, I am not sure anyone would qualify if as working. But yes, I got seriously healthy, I did not get sick for 4 years.
I am doing a “big” Z2 push now, but it’s very mixed activities, most not clearly measurable from a maf test perspective. Also, a lot of weight training now too, so that might screw up my Z2 progress.
Look at this extreme guy that does lots of Zone 2 (This Allan Thrall is pretty smart too)
Also, if you ever decide you want to become Goggins
You should read these guys book below. This guy Jonathan here is one of the smartest coaches/sport scientists I have ever read or talked to. Their company very successfully gets guys to pass the test to become Swat and military elite. So they make seriously bad ass guys more bad ass. When I talked to him on the phone, he told me, “You know my #1 rule is for new guys coming to my program? If you are not going to get good at Zone 2 you can go home now.”
But… When a friend posted something on Reddit asking about Zone 2, to a big cycling group I could still feel the primary belief was “Zwift Races and TR sweet spot.” So even though there are a bunch of us here than understand, it’s obviously very far from a main stream belief.
My regular slow ‘run’ is 6 km at a pace of 9:30 per km. I’s a very slow jog keeping my HR around 115-118 bpm.
And it’s only since about 3 months because before it was more a power walk around the same pace. But I wasn’t able to jog at that low HR. Since i could no longer increase speed while power walking and my HR dropped further, I started jogging/walking. But there is clear improvement, slowly but steadily.
Yes, that was the experience I had as well. Had to mostly walk in the beginning. I eventually got to 8:15 @ 130 back then and 6:55 marathon pace. The interesting thing was I could run a less than 100 bpm at about 10:30 at the peak of my Maffetone period. I did lots of days of 100bpm just as an experiment and also because my wife was slower than me at low HR running.
Now I am 9:30/km for 3k at 120-123 bpm but I am only running about two 20 minute sessions a week but doing lots of other stuff too (rucking, biking…). I don’t even track everything and just watch my HR often without tracking. So I am very close to you. I need to train a bit more to catch up to you
I get to enjoy the treadmill stress test with the ventilator tapes to my face every year for because my cardiologist is a sadist. Having done both that and ekg one I think the ventilator one is a better prediction and if you can talk you are
Aerobic because burning sugar needs a lot of o2. With my bias toward older athletes it’s always better to be low than a smug too high. When are getting the best results from work outs in this order of value: aerobic, anaerobic, vo2max, threshold, sweet spot, tempo
I prescribe almost no sweet spot and let tempo happen only out doors
The rest is 60% aerobic 15 anaerobic, 10% v02max, 10%, threshold 5% over 18 week block. Sometimes if someone is an aerobic mess I will give them 3 weeks of only aerobic + threshold to break them down but that depends on their mental strength which has to be high 3setd of 9x9 at threhold is something only the really strong can handle at the brain gate. That’s basically an ftp race hiding as interval training
For the most part too much threshold and sweet spot leads to frustration for the rider and failed workouts
I rarely do anything higher then over-unders during training. Just because I find it to taxing. I will go all out on outdoor group rides. Must be a motivation issue.
Starting winter base now. Lots of aerobic running (jogging, 5-6 times a week, 45-60 min per session walking my dog), 2 or 3 LIT indoor rides (70-120 min) and one tempo ride. This will be my routine for the whole winter, only the tempo ride will evolve to sweetspot, threshold, over-under.
Must say that I don’t race and my main goals for the season are all long days in the saddle. 8-10 hours, 200-260km, one absolutely flat in the NL and 2 others on rolling terrain.
Long time user of indoor training. Past 5 or so years, proponent of the PoL model. Which has kind of organically adjusted to me, keeping with principals.
A few years back I really struggled to understand the LT1 defined area and even to this day have numerous notes, with numerous calculations all alluding to the correct and golden number( I went so far down the rabbit hole)
Anyhow, unlike most athletes, (safe to say pro athletes have coaches to save them from OTS) I needed to evaluate my life and overindulgence of training and look at holism as a constant. It came following indicators of a developing myopathy and as aforementioned, OTS. Despite what the forums suggest, I would argue it’s fairly easy to send an amateur down there. When you consider, the psychological, cognitive and physical toil of work, life and fitness.
I digress, I started using HRV as a proxy for understanding my recovery. And although this worked reasonably well, I struggled to maintain a’just right’ approach.
I alluded to HRV, found Whoop and immediately got rid and found Marco Altini and HRV4training (still use to this day)
Marco had really done a lot of good quality work in HRV and indeed has had some links with Dr Seiler. Which has led to him developing HRV logger. Very basic experimental app but has allowed to develop
It has been awhile since I’ve read up on MAF, so correct me if I’m wrong.
MAF was designed around runners. And your running HR is going to be higher than your cycling HR for the same zone. I was told/read somewhere to -10 all of my HR zones when comparing running and cycling.
If you’re using regular MAF to determine cycling zones should it not start with -10 in the calculations?
My aerobic zone for running is 120-130. For the same effort cycling it’s usually 108-118.
We had a second discussion around this but the general concensous is maybe in a sport you train more in, you could have a different MAF HR for a sport you don’t train as much in. Maffetone trained triathletes and never set a different target HR for different sports.
Here is our other discussion on this.
So I would guess everyone is a bit different in different sports, I would think monitoring your breadth and ability to talk during the activities might paint a clearer picture if you have a noticeable difference.
 So I see this as Maffetone saying their is a clear relationship between HR and RQ. I have not seen San Milan talking about RQ, and to my limited brain since we are talking about fat burning that is the most obvious indicator.
So I see this as Maffetone saying their is a clear relationship between HR and RQ. I have not seen San Milan talking about RQ, and to my limited brain since we are talking about fat burning that is the most obvious indicator.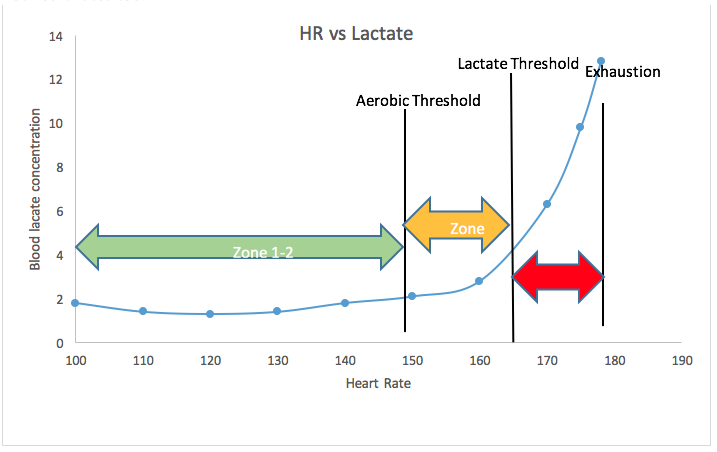

 .
.
