Yes I subscribed to Whoop for 18 months and compared it side by side to Garmin and Garmin resting HR was good enough for me. Garmin sleeping HRV is fine as well. I recover from training fairly poorly, or moderately at best, but I tested peptides for example and that can be a serious recovery booster. I am always working on optimizing stress, with or without consistent training. I think Oura is the best choice but I don’t want to buy anything either, I feel like I have a solid enough understanding and Garmin watch is good enough for my life. If I get more serious about training some day maybe more will make sense.
After 10 days of my participations in discussion about New AlphaHRV program (DFA a1 + Respiration Rate) on intervals forum, it seems that my arguments (based on existing research and my own, small tests related to ECG sampling frequency and sensitivity to artifacts) are being ignored. For the moment, I’m not banned, but all others (but @MedTechCD) are already ‘believers’ and prefer to ignore evidence.
http://www.muscleoxygentraining.com/search?q=frequency would be a reference for AlphaHRV developers: just those two tables after " How did the error correction methods effect the HRV parameters?" section. SD1 set of parameters in 60 - 100% zone of intensity, after artifacts correction (in that respect Kubios correction is not brilliant) have 20-22% bias. Mean based correction gives 10-12% bias.
Bruce continues to investigate the bias problem in his 2019 post and one of conclusions is:
- According to the study by Giles and Draper, RMSSD, LF:HF ratio, SD1, and
SampEn at high (60% + VO2max) exercise intensities will be problematic.
@MedTechCD: you tried to make sens with RR parameters (SD1 a1) on Excel spreadsheet, you said that you switched to NeurKit2 few days ago, and you spent already a lot of time to make sense from training data. I’m sorry, you may think that I’m kind of ‘saboteur’, but I think it is better to have a clear warning and adjust one’s research.
Yes, this is so common. Really I or most of us do the same thing. Ignore the articles that don’t align with our current beliefs uness they happen to be strong enough to shift our beliefs. In hearing about dfa-a1, I was worried about the accuracy of HRV at higher intensities myself. In the past, with my limited N=1 researched showed too much randomness. HRV had to be tightly controlled to be useful for me.
I know in the past Simon at iThlete was one of the biggest leaders in HRV (the original HRV guy). I talked to him before and he is very helpful and loves to talk HRV. I remember in the past he did not feel HRV at higher intensity efforts was useful, it would be interesting to know if he changed his perspective. You could probably reach out to him if you want to learn more.
Thank your for hints about HRV ‘researchers’ (I mean Simon). It seems that there is still a lot of HRV parameters (~ 80%) not being highly sensitive to artifacts correction.
Wearables + HRV may be linked to the smell of ‘big money’:
Few days ago on Google Patents I’ve seen authors of a recent article about ECG signal reconstruction patenting their method (using wavelets) and putting in their preamble numbers about wearable devices potential for healthcare: It was around 40 bilions of USD.
Yesterday, while wandering over ECG material available on net, I stumbled upon “Hurst’s The Heart” book. In “CHAPTER 13: ELECTROCARDIOGRAPHIC EXERCISE TESTING by Gregory S. Thomas; Myrvin H. Ellestad” I found what US cardiologists should consider as standard procedure (Exercise equipment):
Exercise testing can be performed with bicycle ergometry or treadmill testing. /…/
Given the low but finite risk of prolonged myocardial ischemia, infarction, or arrhythmia, and of cardiac arrest, a “crash cart” should be immediately available, and supervising clinicians should have the knowledge to use the medications therein. A defibrillator should also be immediately available, and staff should be trained in its use. Laboratory staff should be well versed in the laboratory’s predefined plan to respond to an emergency. In an outpatient facility, this includes an understanding of who will directly attend to the patient, who will record unfolding events, and who will call for emergency medical transport personnel.
Teriffing: I’m always alone at home while doing FTP evaluation or Critical Power Curve discovery, so I’m now warned. 

My thoughts go two ways:
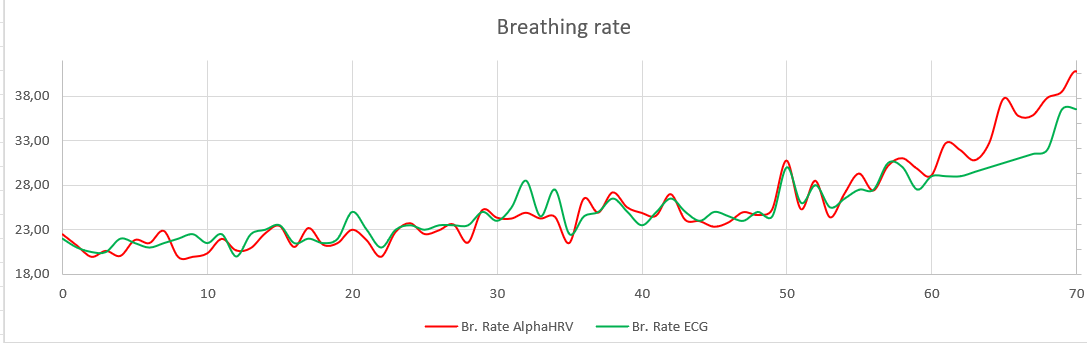
- I honestly believe that the method used by AlphaHRV can give meaningful results. But I’m afraid we will never get there with the limited possibilities of the head units. Although my limited research now gives high credibility to the breathing rate measured by AlphaHRV. I have continued the math in Excell to derive breathing rate from the amplitude changes in the ECG, opposed to the HRV derived breathing rate from AlphaHRV. In 2 of my exercise files (need more time to do a couple more) both traces for breathing rate agree very well.
This was actually not expected. I was doing this to check if the trend was similar and was highly surprised that these methods agreed so well on absolute value. Still need to check this on more of my workouts. - My second thought is that these measurements will never be good enough when used by the modal users. Simply because they don’t understand how much care you need to take to get somewhat valid measurements.
I will do the same investigation on the a1 parameter, with the intent of comparing the results from AlphaHRV-a1 to analysis done with more performant devices like Fatmaxxer (Android Phone), Runalyze and the Fitness Dashboard (Desktop). Mostly interested in Fatmaxxer results because that has proven to be almost on par with Kubios Premium. Purpose is to compare AlphaHRV’s a1 calculated value with the results from Fatmaxxer when inputting the RR stream recorded by the Garmin.
And believe me, you are not ignored will not get banned and are not considered a ‘saboteur’  . It’s just that only a very small group of people know what they are talking about and are willing to invest time and effort. Most other on that thread are there just to ‘profit’ if something comes along. Even to the point that they are slowing us down with questions, remarks all related to poorly acquired data. I’m pretty sure Inigo and Luisma are trying to avoid wasting time with that and that’s why you don’t get a lot of answers from them. I’m curious to see the results they will come up with for a bigger group of athletes. The advantage being that all measurements are being followed up by only 2 guys, thus assuring a stable measurement protocol.
. It’s just that only a very small group of people know what they are talking about and are willing to invest time and effort. Most other on that thread are there just to ‘profit’ if something comes along. Even to the point that they are slowing us down with questions, remarks all related to poorly acquired data. I’m pretty sure Inigo and Luisma are trying to avoid wasting time with that and that’s why you don’t get a lot of answers from them. I’m curious to see the results they will come up with for a bigger group of athletes. The advantage being that all measurements are being followed up by only 2 guys, thus assuring a stable measurement protocol.
They do have a desktop app recalculating the metrics from pure RR stream and that gives them the opportunity to evaluate the results from the IQ-field.
Maybe I’m just wanting too much that this will work, but I can’t ignore that I have a ‘good feeling’ about the way this is evolving.
We came a long way in the mean time. And I still have the impression that you’re not really understanding that HRV and a1 are 2 totally different things.
When it comes to morning HRV, I now have enough proof and experience to say that it is without a doubt very useful. I remember you mentioning in a recent post that RHR does ‘the same’. I absolutely disagree. RHR give you acute or long term information. Anything short term/recent history is completely undetected by RHR alone. HRV does give you that information. But, as I always say, your subjective feelings remain the top number one thing to listen to. The numbers can confirm your feelings or give you a clue and help when you don’t really know what is going on.
For a1, that is a totally different story. At this point, we can’t be sure that something meaningful/useful will result. But we can try to see if it does. As @Retsam says, we must remain skeptical and not ignore research that shows shortcomings of the method.
I’ve done a number of met-cart tests in my professional environment. It was in hospitals or during lectures where the room was full of physiologists/cardiologists.
A full out test like a ramp test can be extremely stressing, if you really push it all the way. I didn’t go that far anymore the last 3-4 years and stop a bit before I would ‘fall of the bike’ or ‘start to throw up’. My ego goes down while my age goes up . A slightly lower VO2max doesn’t bother me.
On the other hand, if you go for a personal best on a climb outdoors, the medical assistance isn’t there either…
In hospitals, these tests are mostly done on people with issues and with way higher risk of crashing. The number of sports tests in hospitals is rather low. Like the meds even stop you when going over 200w and simply say that you are ‘very fit for your age’. In sports centra, it is of course more performance oriented.
My advice: go hard when testing, but stop when you have what you want. A couple of watts difference on an FTP test isn’t going to change your training.
1 Like
I was actually just saying in my case for my purposes, after looking at hundreds of days, lowest night time HR aligns almost 100% to Garmins and Whoops HRV RMSSD based scoring algorythms so I personally don’t need any more then resting HR. Are there uses cases or individuals where that might not be the case, to your point I am sure there is. I am also 100% sure morning HRV works. I realize A1 is something different but ultimately it is using heart rate variability as the underlying change but trying to do it a a much higher heart rate. Again I am not saying it won’t work, I am just skeptical based on my previous, and very limited experience.
I am also not a serious athlete. When I was more consistent, I was a part of a larger group HRV interested group about 10 years ago when HRV was first getting popular, that most individuals saw a direct relationship between an orthostatic and RMSSD as well. That was before 24 hour monitoring devices were around. 24 hour devices make it even easier. HRV is more sensitive, but I don’t see the need for this additional sensitivity in myself.
We will see, at this time it is all speculation. I think tradtional HRV has a much higher success rate of alignment. I would guess A1 is more like SMO2 sensors, works for some, not for others, much more hit or miss. That coming directly from discussing with the guys at Moxy. SMO2 seems to work well for me.
Yeah, I never go very hard on a ramp test. I would say I have at least another minute left in the tank, so I could not agree more. Because I am more of a sprinter profile, ramp tests still over estimate my FTP even stopping a minute early.  I just know I have to drop it about 15% from what I get. Nice ego booster as it is.
I just know I have to drop it about 15% from what I get. Nice ego booster as it is.
Met-cart tests are always ramp tests and in sports medecine, they push you to the limit to get that ‘magic’ VO2max number. Goal is to reach that point in 12-20 minutes step or ramp test, usually 20 or 25w /min.
Most still don’t care a lot about FTP, all that count is VO2max. If you ask for FTP, they simply give you the wattage at VT2 or they take 75% of max power.
I’m satisfied once I have VT1 and VT2. And although the ventilation method in these tests is the Gold standard for determining the thresholds, there is also some debate after every test to exactly pinpoint the numbers…
Best is to have a lactate test done at the same time (that’s not always the case)
I always ask for a csv with the metrics to have a look at myself afterwards.
Yep. Andrea does ramp tests with masks almost everyday for 30 years or so. Mostly pro cyclists, but a lot of no pros as well.
He says ramp is very accurate for Vo2max and you can fairly accurately predict ftp to be between 70-80% of Vo2max for about 90% of the riders. But as you can see that’s a pretty large degree of inaccuracies in FTP but he also says ramp tests are highly consistent from test to test, more so than tests like 20 minute tests. This matches my experience.
I’m also used to check my RHR (but after a couple of hours after training, like [taxing] swimming today). So it is not ‘night after low’, but ‘current’ one. It will return to my day average 2-4 hours later. Then I can do another chunk on the home cycle or the rebouncer. This will be not taxing me, as intensity will be around VT1.
Now, back to Bruce post (Muscle Oxygen Training: DFA a1 as a biomarker of fatigue - article review), he found that comparing DFA short frequency reaction to big effort, after and before, HR while doing easy exercise shows no post-impact and DFA a1 does.
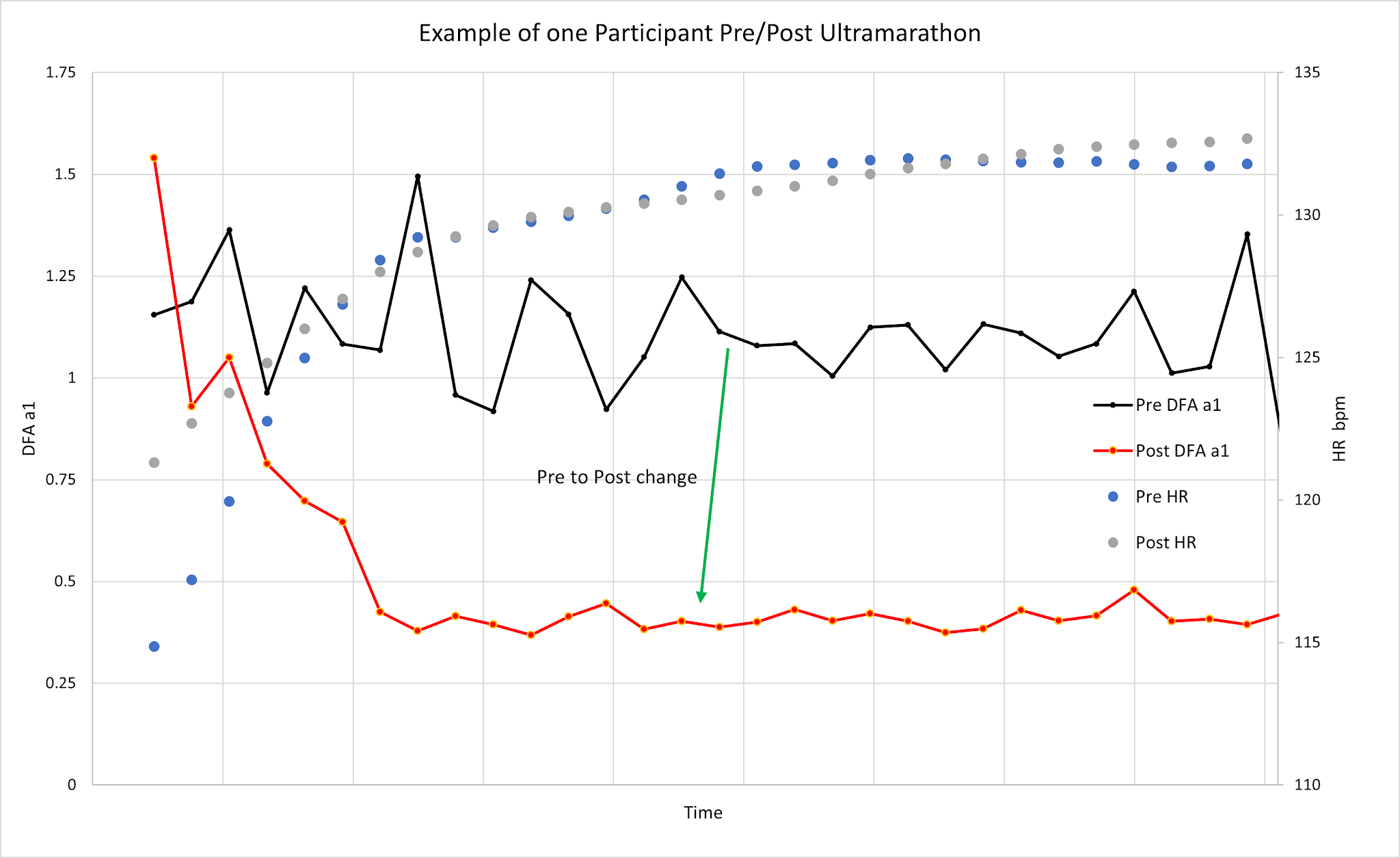
However, HR before that easy exercise for that example is quite higher over 5-10 minutes (see left part of the chart). So myself, without starting that exercise I will know, that I’m ‘not fresh’.
Oh I see. Yes, I never worry about multiple sessions in the day as long as my longer term trend is ok and I don’t appear to be getting sick and am not totally exhausted.
I also see much clearer trend in lowest night time hr than RHR. RHR is not very accurate for me.
I admit I use ‘quick’ method to evaluate reliability of numerical methods to evaluate dynamic system (here it is ANS behavior, reduced to 89 HRV parameters). That heuristic comes from my long experience in designing trading algos: I used / created NN, Genetic Programming, fractals etc. All traders were convinced that adding one more parameter will make them happy and rich. Convincing traders that removing most of parameters can help them to get perhaps 1-2% of edge (mainly on long term), was nearly impossible.. Near all ‘technical indicators’ are cross-correlated and no knowledge can be gained by combining them. Moreover ‘spurious correlation’ in near random data will fool everybody.
You are hinting that RespRate from ECG (not RR) should help to spot the transition point. In my opinion RespRate in ECG is not ‘orthogonal’ (this means ‘independence’) enough to DFA a1 to bring clarity in ‘knee’ detection.
Mr. Taleb (Black swan and other books about randomness) speaks about hormesis, it relates mostly to combined medicine being hurtful, near impossible to predict. Then he suggest replacing current ‘adding to’ model of taking care to ‘suppressing from’ model. I will gladly extend it to other fields.
2 hours of hard swimming, you are tough Is it not obvious after that you are not fresh anyway? I would think if you call something “2-hours of hard” it’s fairly obvious you are not fresh, unless you typically do 6 hours of hard each day then 2 hours might still feel fresh I guess.
I am just trying to understand if there is some value in this immediate feedback. I guess if it pointed you to better fueling or something it could be a help. I am just trying to understand what use cases this actually would make a difference in training rather that just an extra parameter
Oh maybe a dopamine hit? Kind of like a MAF test, immediate feedback you are improving, without needing to take an all out test. I did 300 TSS today and my A1 says I am fresh still?
Well, I said: “… couple of hours AFTER training, like swimming… …” So I take it easy: it is only one hour of swimming, trice w week. ![]() Thank you to jump on the opportunity to make a pun.
Thank you to jump on the opportunity to make a pun.
But really, seeing, just from HR, that you should be OK a couple of hours after an effort instead of 5-6 hours (like 2 months ago), makes you believe that ‘crash cart’ should not be called yet and your body handles better the load.
Parameters from HRV, interpreted by few different led based devices / makers, are nearly useless. In near the same time, I got 8/10 points readiness from one and 95% of stress, 15% of energy from another. Quite a BS. Vendors responses are typical: check that place on your skin is right, or your skin may be too cold, whatever. Or even better: we will give you 5 more ‘parameters’ (for instance ‘coherence’ ![]() ) and this will costs ‘only’ 5 bucks peer month.
) and this will costs ‘only’ 5 bucks peer month.
So again, KISS!
I guess I just see that going severly negative for a single day is not a big problem, it’s the long term trend that is bad. I agree the wrist based sensors are highly inaccurate in many cases but actually in the case of night time statistics it actually aligns very well. So if you are wanting to do scientific comparisons during the day they are worthless. But just using them for many years both Garmin and Whoop statistics seem to align very well to stress. I think the end suggestions are bad but what they present as metrics is good enough to make informed decsions.
I hate monthly fees so am in agreement there. I just felt I had to understand the value, to better understand what role these devices could hold for future iterations of our product. Most people need dead simple or it won’t happen, myself included.
My, now infrequent, tenis partner, 50+, was awaken at 3 AM, by his Apple watch, with a message about ‘immediate action is necessary’. His HR went below 34 BMP.  Hi has long lasting bradycardia (and is not endurance athlete at all). Now he plans to go to cardiologist which will possibly add a ‘heart pacer’ to his Apple watch. End of smart watch messages while asleep.
Hi has long lasting bradycardia (and is not endurance athlete at all). Now he plans to go to cardiologist which will possibly add a ‘heart pacer’ to his Apple watch. End of smart watch messages while asleep.
[I’m still upset with Kubios artifacts correction algo tested in NeurKit2: I need to decompress]. Back to bradycardia: I’m musing about genetic link of some people to bears. While hibernating, their HR is about 10 BMP, body temperature is about 32-33 C and it is harmless for 3-4 months. So human bradycardia in the range 20-30 may also be harmless to people (is winter the trigger of it?), but nobody wants to take the risk. But now, security of experiment would be granted by the Apple smart watch, as being awaken with the message ‘WAKE UP OR…’ should prevent further drop.
Claude, I realized I like your thinking on this breathing rate. I would love to see a graph of breathing rate to power (I have only looked at nightime averages, nothing more). I have a few devices, I would like to test this unless you have some data. Probably a ramp test with 5 minute ramps would be ideal.
I guess at say 110% of FTP your breathing rate will keep going up until you crash… even when power stays flat. It would be interesting to see the point at which power and breathing rate don’t decouple. I would guess might be highly suspect to daily changes like HR vs Power and some where around LT1? I would think higher but really a total guess.
For regular joes, that have a spin bike or people that want to train by RPE, I wonder if their is an interesting association there I would guess RPE and breathing rate are connected.